NOTE
* IAW USSOCOM Sanitization Protocol for Historical Articles on Classified Current Operations, pseudonyms are used for majors and below who are still on active duty, unless names have been publicly released for awards/decorations or DoD news release. Pseudonyms are identified with an asterisk. The eyes of personnel in photos are blocked out when not covered with dark visors or sunglasses, except when the photos were publicly released by a service or DoD. Source references (end notes) utilize the assigned pseudonym.
SIDEBAR
Results of the
‘Nili Experiment’
- Validated the VSO concept
- Improved the security of Nili and surrounding districts
- Established the practicality of combining CA and PSYOP elements with SF ODA
- Established good rapport between the coalition and Hazara people
- Improved people’s view on GIRoA legitimacy
- Highly visible success with tangible public results
- Provided a wealth of information on how to establish and support VSO in the field
- Established a baseline of information on establishing the Afghan Local Police
- The experiences of ODA 7224 helped shape the VSO program
Factors Contributing to
ODA 7224 Success
- Critical Examination of Historical Precedents
- Fully Understood Historical, Cultural, Economic, Ethnic, Religious Background of People
- Mature, Experienced, Stable Team
- Honest Self-Assessment and Ability to Communicate with Higher Commands
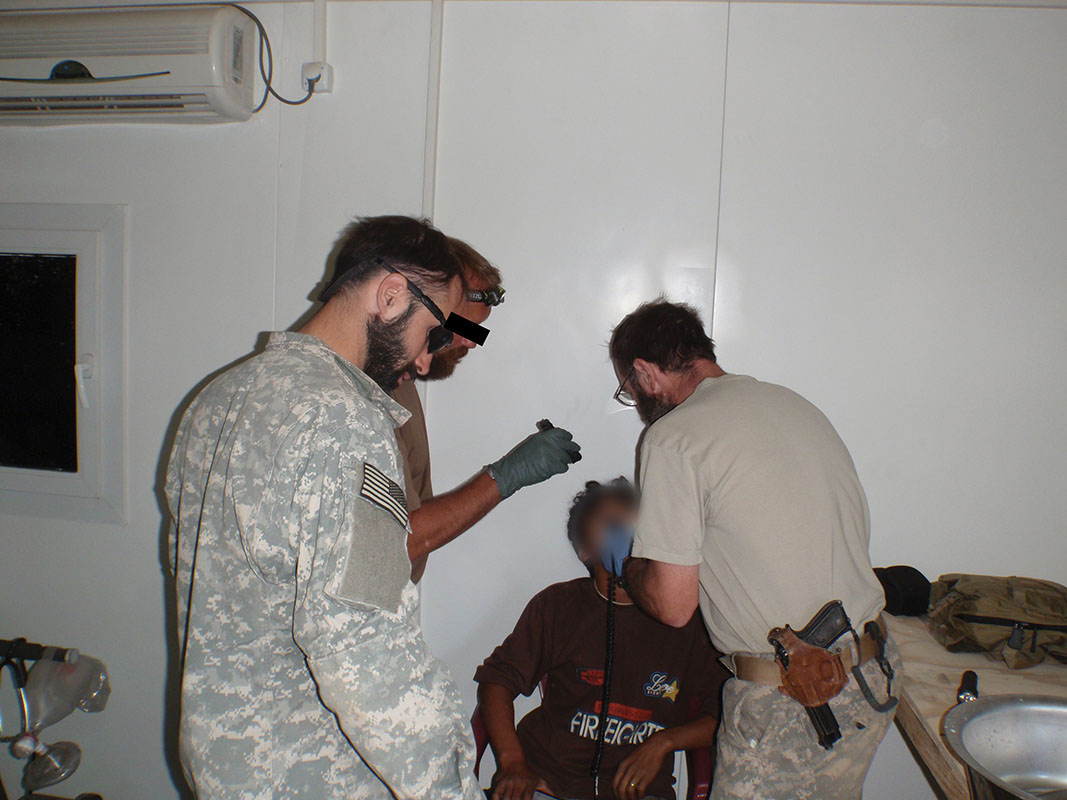
When he first saw the child in the long line of patients, Sergeant First Class (SFC) Dan A. Marvin*(pseudonym), junior Special Forces (SF) Medical Sergeant, knew that this was the most serious case he would see today and that the boy might not survive. Malik, about two years old, had fallen off the roof of his house a few days earlier and his condition had gradually declined. Now he was listless and unresponsive, with a massive bulge protruding from his skull. SFC Marvin* diagnosed hematoma and brain trauma. He “didn’t appear to see anything, he wouldn’t track with his eyes, couldn’t get much of a response from his pupils” said Marvin*.1 The child had paralysis on the left side of his body, a sympton that was consistent with the damage to the right side of the skull. Malik’s desperate father, hearing that Americans were providing medical treatment in Nili village, carried his lethargic child about 50 kilometers hoping they could help. As the soldiers of Operational Detachment - Alpha (ODA) 7224 realized the seriousness of Malik’s injuries, they moved into action to save his life.2


SFC Marvin* and the senior SF Medical Sergeant, SFC Josiah Monza*, stabilized the child, cleaned his injuries, and made him comfortable. Other team members explored options to evacuate Malik for major trauma surgery. Without surgery the boy would die. The Afghans had no hospital with the capability to perform delicate surgery outside Kabul, and the closest military facility with the means to treat Malik’s injuries was in Kandahar, 400 kilometers to the south. And neither the district nor province officials had the means to medically evacuate (MEDEVAC) a patient that distance. Coalition forces were initially reluctant to evacuate an Afghan not injured in combat. When SFC Marvin* notified the ODA Team Leader, Captain (CPT) Mike L. Bourne* Jr., of the situation, Malik’s care became a priority. Their actions (or inaction) were being judged by the people of the region. Since the ODA was to forge good relationships with the villagers, Malik’s critical condition was an ideal platform.3
Working through the higher headquarters, the senior Weapons Sergeant, SFC Brad D. Rendition*, a qualified Joint Tactical Aircraft Controller (JTAC), arranged for a passing helicopter to fly Malik and his father to Kandahar. On arrival, Malik was rushed to a U.S. military surgical unit where a neurosurgeon operated to relieve the pressure on his brain and repair the damage. The operation took place just in time; the swelling subsided and he became more alert and aware of his surroundings. Within days the paralysis began to dissipate, and feeling and mobility returned to his left side. Malik’s case attracted the attention of Cable News Network (CNN) commentator and neurosurgeon Dr. Sanjay Gupta, who had been reporting on the war and visiting medical facilities. Dr. Gupta saw the child, heard the story, and publicized Malik’s splendid recovery. He also accompanied the boy and his father back to Nili. International television covered the event, highlighting the life-saving efforts of the SF ODA. The boy’s father, Khodadad, was ecstatic: “God answered our prayers, God sent someone to save my son.” The act of kindness bolstered trust and earned the esteem of the local villagers. These Special Forces soldiers could be counted on in time of need.4
This article examines Army SOF’s first deliberate experiment with Village Stability Operations (VSO) in Afghanistan, an event that marked a dramatic change in the SOF role. It explains how the concept came about, its goals, and what SOF planners were hoping to achieve. In particular, it focuses on ODA 7224’s actions in that situation and how their experiences shaped the future expansion of the program. How ODA 7224 prepared and adapted were key. The SF soldiers thrived on the challenges of the new mission. Despite limited information about their area they soon became experts on the region. They anticipated requirements, understanding the need for integrating Civil Affairs and Psychological Operations into their efforts. The ODA exercised good initiative and anticipated needs for assistance. They also provided detailed feedback on progress to their higher command staff, thereby sharing ‘lessons learned’ so others could benefit. The success achieved by ODA 7224 caused a rapid growth of SF teams doing VSO missions throughout Afghanistan. ODA 7224 set the standards for individuals and teams. Here’s what they did to shape and influence village stability operations as it happened.